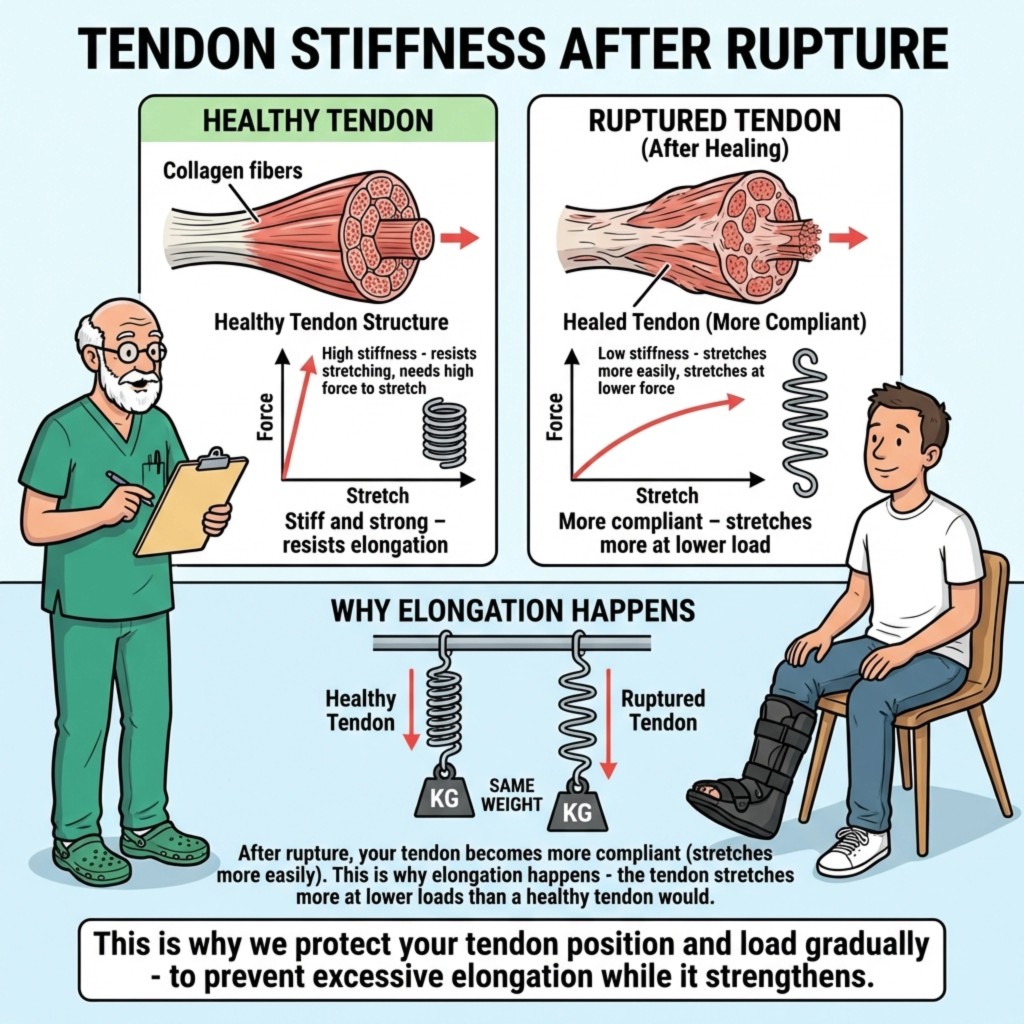
If you picture a healthy Achilles tendon as something tightly organized — collagen fibres lined up like strong cable — tendon stiffness is partly what stops everyday steps from stretching it out like chewing gum. After an Achilles tendon rupture, the new tissue that bridges the tear is initially messier, more watery, and more compliant. In plain English: Achilles tendon elongation risk rises because healing tissue pulls longer under the same loads than your original tendon did. Clinicians emphasise boot position, wedge schedules, and controlled loading to keep tendon ends close while that tissue stiffens — not because they enjoy rules, but because mechanical protection aligns with how stretchy healing tendons behave in research.
For the wider picture — dramatic re-rupture versus quiet elongation, numbers, and what patients feel — see Achilles re-rupture versus tendon elongation.
Contents
- Key takeaways
- Stiff versus compliant — the spring analogy
- Healthy tendon versus healed tendon (what changes)
- Gap on scan versus tendon ends meeting in the boot
- What research adds (without drowning you in maths)
- What this means for your recovery
- Frequently asked questions
- References
Key takeaways
- Healing tendon after Achilles rupture behaves like a softer spring early on — it stretches more under ordinary loads (more compliant) than intact tendon (stiffer).
- That mechanical reality is why excessive dorsiflexion (toes pointed up early) or forcing stretches worries teams: the load lengthens immature collagen more easily — Achilles tendon elongation.
- Imaging gap size matters, but clinicians also care whether ends sit together under the plantarflexion (pointed) angles your pathway uses — approximation is functional, not just a millimetre readout.
- Controlled weight-bearing, respecting wedge progression, night protection, and late-game strength work are your practical tools — movement is allowed, just metered.
- Worried about a snap, buckling, or sudden pain after a mishap → seek urgent assessment (re-rupture is uncommon overall but serious).
Stiff versus compliant — the spring analogy
Think of stiffness as how steep the line is when you plot stretch versus force:
- Stiff tendon (healthy): you need more force for each bit of lengthening — tissue resists stretch.
- Compliant tendon (healing early): the same modest force produces more lengthening — it yields.
That is exactly what mechanical studies suggest after rupture: injured tendons can show lower dynamic stiffness markers on imaging alongside greater length than the opposite side early in rehab. It does not mean you are doomed; it explains why protection and gradual progression are rational, not punitive.
During the proliferative bridging weeks (roughly weeks 3–6 — see our timeline and early healing biology), new collagen forms a temporary scaffold. It tolerates protected load well but still elongates more easily if repeatedly tensioned into dorsiflexion (toes-up) before your timetable allows.
Healthy tendon versus healed tendon (what changes)
| Aspect | Healthy tendon | Healed tendon (early / mid rehab) |
|---|---|---|
| Collagen pattern | Tightly bundled, orderly | Initially more wavy / disorganised → matures toward order over months |
| Mechanics (simple view) | Stiff, resists elongation under step loads | More compliant, lengthens more per step / per load episode unless protected |
| What you notice | You rarely think about tendon length walking | Slack length can blunt plantarflexion (push-off) if excessive — strength, walking rhythm, sport readiness affected in some athletes |
| What helps | N/A — keep it intact | Boot angle, accurate heel wedges, controlled loading, later structured strengthening |
Residual callus thickness visible on ultrasound is normal and different from the question of excessive slack length. Our broader piece on calf power explains how elongation interacts with heel-rise metrics: long-term strength after rupture.
Gap on scan versus tendon ends meeting in the boot
Ultrasound gap readings get anxious airtime online. They are useful, yet clinical positions rightly treat gap as one factor among many: activity goals, tendon quality, adherence, footwear weaning, and rehab all sway outcome.
Approximation means bringing ends near consistently in the posture your surgeon or therapist targets — historically equinus-heavy (pointed) early, then phased reduction with wedges or a hinge. If your images look “wide” yet you are splinted with ends held close in boot plantarflexion, that may still be workable; mirror-image decisions belong to your team — do not micromanage numbers from Reddit threads alone.
Protocols differ; principles repeat: do not sprint the angle schedule (wedge rationale), maintain ankle posture consciously when standing or transferring (foot position primer), and negotiate sleep safety honestly — some patients add a clinician-approved night splint when boot sleep fails.
What research adds (without drowning you in maths)
-
Ultrasound-derived stiffness rises and length evolves during the first months. Twenty-seven rupture patients scanned at 4–24 weeks showed lower dynamic shear modulus, larger cross-section, and longer tendon on the torn side versus the healthy side — metrics that trended toward recovery over time (Zellers et al.). Early structural measures correlated with later gait and heel-rise symmetry, implying early protection has downstream leverage.
-
Time-dependent lengthening (‘creep’) under steady load persists for months. In an operative pilot series with bead markers, tendon separation under steady calf loading showed large creep (several percent strain across minutes) around seven weeks, shrinking toward week 19 — consistent with healing tissue behaving more viscous and stretch-prone early (Aspenberg & Schepull). Non-operative pathways are not mapped bead-for-bead in that paper, but the same mechanical idea motivates protected angles and gradual loading broadly.
-
Strain versus force gradually normalises. Stereogrammetric tendon strain experiments (small RSA cohort after surgical repair) described greater stretch per 100 N at six weeks, improving toward one year, and early modulus trends linked with later heel raise performance (Schepull et al. pilot series).
-
Elongation is widespread on imaging yet symptom links vary. A large systematic review pooled measurable lengthening in many healed tendons — mean imaging spreads up to roughly three centimetres across cited cohorts — with balanced evidence tying elongation tightly to questionnaire scores versus clearer patterns in biomechanical laboratory measures (Diniz et al.).
These studies do not mean micromanaging every tenth of a millimetre; they reinforce training structure: protect length while tissue stiffens, then progressively load calf capacity through criteria-based physiotherapy. Our progressive recovery course mirrors that phased mindset for patients needing a narrative scaffold.
What this means for your recovery
Do:
- Wear your boot whenever upright until cleared; treat each wedge removal date like a labelled medicine dose — no DIY acceleration.
- Walk within prescriptions (many pathways allow early protected weight-bearing); movement supports circulation and morale if done safely.
- Start supervised physiotherapy roughly weeks 3–6 if referred — concentrate on hip, calf activation inside allowed angles, balance, gait quality.
- Discuss blood thinner adherence and clot warning signs openly if prescribed — parallel issue but part of pragmatic early weeks (clot-risk article).
Avoid:
- Forced stretching or leaning into max dorsiflexion before sanctioned.
- Competitive mileage hikes, sprinting errands, barefoot “tests,” or hopping stairs early.
- Swapping hinge angle because a friend’s protocol differed — comparison is meaningless unless your surgeon agrees.
Red-flag after trauma or stumble: audible snap, abrupt slackness, inability to toe-off unexpectedly, escalating pain/swelling → Emergency / fracture clinic urgency.
Frequently asked questions
What does it mean when doctors say my healing Achilles is “more compliant”?
Compliance (inverse of stiffness) means the tendon lengthens more for each unit of tensile force. Casual translation: it behaves softer temporarily. Healing tissue should toughen progressively; clinicians limit dangerous stretch directions until stiffness catches up functionally.
Is imaging gap size the only thing that matters for tendon length?
No. Imaging helps, but clinicians integrate exam, desired plantarflexed posture, and clinical approximation assumptions. Gap is informative, not solitary — fixation on digits without context breeds anxiety rather than smarter loading.
Will my tendon eventually become as stiff as before?
Possibly partly — evidence suggests persistent mechanical differences can remain versus the uninjured tendon in lab studies — yet sport-level and recreational function still returns commonly when rehab targets controlled strength.
What should I avoid in early rehab to reduce elongation risk?
Unprotected dorsiflexion, early aggressive stretching, boot removal escapades, DIY wedge acceleration, reckless inclines/long strides — essentially anything that loads a thin, stretch-prone scaffold eccentrically sooner than timetable allows.
How is elongation risk different from re-rupture risk?
Re-rupture tends to announce itself dramatically and remains statistically uncommon (~3–5% broadly). Elongation can occur quietly, preserving continuity but shortening effective calf leverage. Separate fears, intertwined prevention: controlled progression. Read both stories in Achilles re-rupture versus tendon elongation.
References
-
Zellers JA, Cortes DH, Pohlig RT, Silbernagel KG. Tendon morphology and mechanical properties assessed by ultrasound show change early in recovery and potential prognostic ability for 6-month outcomes. Knee Surg Sports Traumatol Arthrosc. 2019;27(9):2831-2839. DOI: 10.1007/s00167-018-5277-8
-
Aspenberg P, Schepull T. Substantial creep in healing human Achilles tendons. A pilot study. Muscles Ligaments Tendons J. 2015;5(3):151-155. DOI: 10.11138/mltj/2015.5.3.151 (PMC free article)
-
Schepull T, Kvist J, Andersson C, Aspenberg P. Mechanical properties during healing of Achilles tendon ruptures to predict final outcome: A pilot Roentgen stereophotogrammetric analysis in 10 patients. BMC Musculoskelet Disord. 2007;8:116. DOI: 10.1186/1471-2474-8-116
-
Diniz LO, Pacheco J, Guerra-Pinto F, et al. Achilles tendon elongation after acute rupture: is it a problem? A systematic review. Knee Surg Sports Traumatol Arthrosc. 2020;28(12):4011-4030. DOI: 10.1007/s00167-020-06010-8
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1564-1571. DOI: 10.1177/0363546512447926
Primary source: Zellers JA, Cortes DH, Silbernagel KG, et al. (2019). Tendon morphology and mechanical properties assessed by ultrasound show change early in recovery and potential prognostic ability for 6-month outcomes
