If you are in later-stage Achilles rehab, single-leg heel raises are one of the most useful milestones. They mark the shift from basic capacity building to functional performance: can your recovering tendon and calf handle bodyweight through one side with control?
Clinicians often use the ability to complete roughly 15 controlled single-leg reps on flat ground as an early proxy for readiness to progress load. But that is not the finish line. In many pathways, the longer-term benchmark is closer to 25+ high-quality reps with good symmetry and heel-rise height.
The key is progression sequence. Not every harder variation is better at every stage.
Contents
- Key takeaways
- Why single-leg heel raises matter
- A practical progression ladder
- Why deficit raises need timing
- What this means for your recovery
- Frequently asked questions
- References
Key takeaways
- Single-leg heel raises are a core indicator of calf-tendon function after Achilles rupture.
- Around 15 controlled flat-ground reps can be a useful early progression checkpoint.
- Many protocols still target 25+ quality reps as a stronger later-stage capacity marker.
- Early progression should usually be double-leg -> single-leg flat ground -> loaded flat ground.
- Deficit (off-step) raises increase dorsiflexion demand and are often delayed until strength and control are established.
- The priority is load progression before stretch-heavy positions to reduce elongation risk.
Why single-leg heel raises matter
Single-leg heel raises are not just a gym test. They stress the same system you need for daily push-off: calf muscle force, tendon stiffness, and neuromuscular control.
Research on Achilles rupture outcomes consistently links heel-rise performance with tendon behavior over time. Silbernagel and colleagues showed that greater tendon elongation was strongly associated with poorer heel-rise height in recovery. In plain terms: if the tendon heals long, you often lose push-off quality.
That is why many rehab teams track heel-raise capacity carefully and avoid rushing into high-strain variations too early.
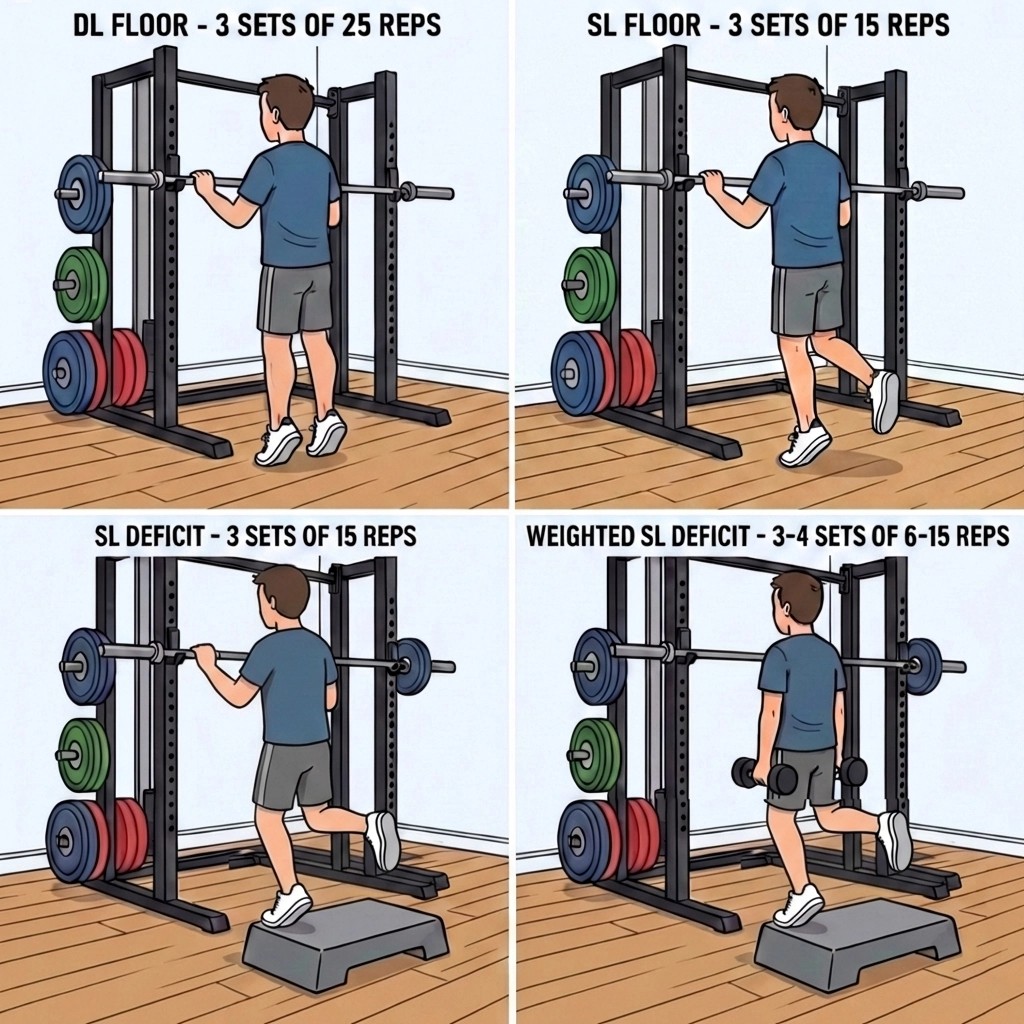
A practical progression ladder
Your infographic maps well to how many clinicians sequence this phase:
| Stage | Typical prescription style | What to focus on |
|---|---|---|
| Double-leg floor raises | Often around 3 x higher reps | Build baseline calf endurance with controlled tempo |
| Single-leg floor raises | Often around 3 x moderate reps | Maintain full control, clean height, no trunk sway |
| Weighted single-leg floor raises | Lower rep ranges with external load | Increase load while preserving form and range |
| Deficit/step variations | Added later when criteria are met | Expand ROM only after adequate strength/stiffness |
Rep schemes vary by clinician and stage, but quality rules are similar:
- Smooth rise and controlled lower (no bouncing).
- Keep load through the first and second toe, not rolling out.
- Match side-to-side heel-rise height as closely as possible.
- Stop if form collapses.
If you are still in earlier transition phases, this sits on top of the boot-off timeline discussed in walking boot removal timing and the broader progression logic in Achilles rupture rehabilitation FAQs.
Why deficit raises need timing
Deficit heel raises (off a step) can be useful later, but they increase dorsiflexion demand and tendon strain. In a recovering tendon, that extra stretch exposure is not always the right first move.
A safer pattern for many patients is:
- Master flat-ground single-leg raises.
- Add external load while staying on flat ground.
- Introduce deficit range later, when clinician criteria are met.
This aligns with the principle used across Achilles pathways: restore strength and stiffness before high-strain positions.
It also fits with site-wide guidance to avoid aggressive early stretching in recovery. If your tendon is irritated, stiff, or your gait worsens after a new variation, progression may be ahead of tissue capacity.
For bigger-picture context on persistent deficits, see long-term strength after Achilles rupture.
What this means for your recovery
Do:
- Use a structured ladder rather than random exercise jumps.
- Treat 15 clean reps as a checkpoint, not graduation.
- Keep working toward higher-quality capacity (often 25+ reps) over time.
- Add load gradually and keep movement quality non-negotiable.
Avoid:
- Chasing range before strength.
- Starting off-step deficit work too early.
- Ignoring next-day swelling, pain, or reduced heel-rise height.
If symptoms spike, de-load and talk to your physiotherapist. Progression speed should follow tendon response, not social media timelines.
For stage-based education that ties these milestones together, the recovery course can help.
Frequently asked questions
Why are single-leg heel raises such an important milestone?
They are a practical way to test whether one calf-tendon unit can generate and control enough force for real-world push-off.
Is 15 reps enough, or should I aim for 25 reps?
Think of 15 as an early checkpoint and 25+ as a stronger later target in many protocols.
Should I do heel raises off a step early?
Usually no. Early work is commonly done on flat ground to prioritize load tolerance before extra dorsiflexion demand.
When should I add weight?
After clean flat-ground single-leg performance is consistent, with no symptom flare and good control.
What signs mean I progressed too quickly?
Persistent next-day pain, swelling, reduced heel-rise quality, or worsening limp usually mean current load is too high.
References
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1568-1575. https://doi.org/10.1177/0363546512447926
-
Silbernagel KG, Gustavsson A, Thomeé R, Karlsson J. A new measurement of heel-rise endurance with the ability to detect functional deficits in patients with Achilles tendon rupture. Knee Surg Sports Traumatol Arthrosc. 2010;18(2):258-264. https://doi.org/10.1007/s00167-009-0889-7
-
Zellers JA, Carmont MR, Grävare Silbernagel K. Defining Components of Early Functional Rehabilitation for Acute Achilles Tendon Rupture: A Systematic Review. Orthop J Sports Med. 2019;7(11):2325967119884071. https://doi.org/10.1177/2325967119884071
-
Zellers JA, Carmont MR, Grävare Silbernagel K. Heel-Rise Height Deficit 1 Year After Achilles Tendon Rupture Relates to Changes in Ankle Biomechanics 6 Years After Injury. Am J Sports Med. 2018;46(11):2670-2677. https://doi.org/10.1177/0363546517717698
Primary source: Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture
